NEET MDS Lessons
Orthodontics
Retention
Definition: Retention refers to the phase following active orthodontic treatment where appliances are used to maintain the corrected positions of the teeth. The goal of retention is to prevent relapse and ensure that the teeth remain in their new, desired positions.
Types of Retainers
-
Fixed Retainers:
- Description: These are bonded to the lingual surfaces of the teeth, typically the anterior teeth, to maintain their positions.
- Advantages: They provide continuous retention without requiring patient compliance.
- Disadvantages: They can make oral hygiene more challenging and may require periodic replacement.
-
Removable Retainers:
- Description: These are appliances that can be taken
out by the patient. Common types include:
- Hawley Retainer: A custom-made acrylic plate with a wire framework that holds the teeth in position.
- Essix Retainer: A clear, plastic retainer that fits over the teeth, providing a more aesthetic option.
- Advantages: Easier to clean and can be removed for eating and oral hygiene.
- Disadvantages: Their effectiveness relies on patient compliance; if not worn as prescribed, relapse may occur.
- Description: These are appliances that can be taken
out by the patient. Common types include:
Duration of Retention
- The duration of retention varies based on individual cases, but it is generally recommended to wear retainers full-time for a period (often several months to a year) and then transition to nighttime wear for an extended period (often several years).
- Long-term retention may be necessary for some patients, especially those with a history of dental movement or specific malocclusions.
Forces Required for Tooth Movements
-
Tipping:
- Force Required: 50-75 grams
- Description: Tipping involves the movement of a tooth around its center of resistance, resulting in a change in the angulation of the tooth.
-
Bodily Movement:
- Force Required: 100-150 grams
- Description: Bodily movement refers to the translation of a tooth in its entirety, moving it in a straight line without tipping.
-
Intrusion:
- Force Required: 15-25 grams
- Description: Intrusion is the movement of a tooth into the alveolar bone, effectively reducing its height in the dental arch.
-
Extrusion:
- Force Required: 50-75 grams
- Description: Extrusion involves the movement of a tooth out of the alveolar bone, increasing its height in the dental arch.
-
Torquing:
- Force Required: 50-75 grams
- Description: Torquing refers to the rotational movement of a tooth around its long axis, affecting the angulation of the tooth in the buccolingual direction.
-
Uprighting:
- Force Required: 75-125 grams
- Description: Uprighting is the movement of a tilted tooth back to its proper vertical position.
-
Rotation:
- Force Required: 50-75 grams
- Description: Rotation involves the movement of a tooth around its long axis, changing its orientation within the dental arch.
-
Headgear:
- Force Required: 350-450 grams on each side
- Duration: Minimum of 12-14 hours per day
- Description: Headgear is used to control the growth of the maxilla and to correct dental relationships.
-
Face Mask:
- Force Required: 1 pound (450 grams) per side
- Duration: 12-14 hours per day
- Description: A face mask is used to encourage forward growth of the maxilla in cases of Class III malocclusion.
-
Chin Cup:
- Initial Force Required: 150-300 grams per side
- Subsequent Force Required: 450-700 grams per side (after two months)
- Duration: 12-14 hours per day
- Description: A chin cup is used to control the growth of the mandible and improve facial aesthetics.
Types of Springs
In orthodontics, various types of springs are utilized to achieve specific tooth movements. Each type of spring has unique characteristics and applications. Below are a few examples of commonly used springs in orthodontic appliances:
1. Finger Spring
- Construction: Made from 0.5 mm stainless steel wire.
- Components:
- Helix: 2 mm in diameter.
- Active Arm: The part that exerts force on the tooth.
- Retentive Arm: Helps retain the appliance in place.
- Placement: The helix is positioned opposite to the direction of the intended tooth movement and should be aligned along the long axis of the tooth, perpendicular to the direction of movement.
- Indication: Primarily used for mesio-distal movement of teeth, such as closing anterior diastemas.
- Activation: Achieved by opening the coil or moving the active arm towards the tooth to be moved by 2-3 mm.
2. Z-Spring (Double Cantilever)
- Construction: Comprises two helices of small diameter, suitable for one or more incisors.
- Positioning: The spring is positioned perpendicular to the palatal surface of the tooth, with a long retentive arm.
- Preparation: The Z-spring needs to be boxed in wax prior to acrylization.
- Indication: Used to move one or more teeth in the same direction, such as proclining two or more upper incisors to correct anterior tooth crossbites. It can also correct mild rotation if only one helix is activated.
- Activation: Achieved by opening both helices up to 2 mm at a time.
3. Cranked Single Cantilever Spring
- Construction: Made from 0.5 mm wire.
- Design: The spring consists of a coil located close to its emergence from the base plate. It is cranked to keep it clear of adjacent teeth.
- Indication: Primarily used to move teeth labially.
4. T Spring
- Construction: Made from 0.5 mm wire.
- Design: The spring consists of a T-shaped arm, with the arms embedded in acrylic.
- Indication: Used for buccal movement of premolars and some canines.
- Activation: Achieved by pulling the free end of the spring toward the intended direction of tooth movement.
5. Coffin Spring
- Construction: Made from 1.2 mm wire.
- Design: Consists of a U or omega-shaped wire placed in the midpalatal region, with a retentive arm incorporated into the base plates.
- Retention: Retained by Adams clasps on molars.
- Indication: Used for slow dentoalveolar arch expansion in patients with upper arch constriction or in cases of unilateral crossbite.
Growth is the increase in size It may also be defined as the normal� change in the amount of living substance. eg. Growth is the quantitative aspect and measures in units of increase per unit of time.
Development
It is the progress towards maturity (Todd). Development may be defined as natural sequential series of events between fertilization of ovum and adult stage.
Maturation
It is a period of stabilization brought by growth and development.
CEPHALOCAUDAL GRADIENT OF GROWTH
This simply means that there is an axis of increased growth extending from the head towards feet. At about 3rd month of intrauterine life the head takes up about 50% of total body length. At this stage cranium is larger relative to face. In contrast the limbs are underdeveloped.�
By the time of birth limbs and trunk have grown faster than head and the entire proportion of the body to the head has increased. These processes of growth continue till adult.��
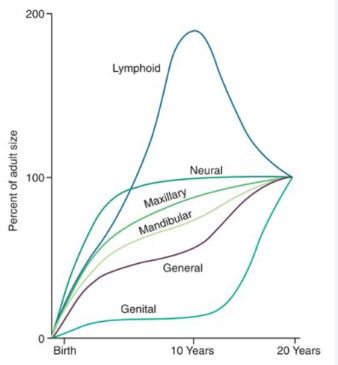
SCAMMON�S CURVE
In normal growth pattern all the tissue system of the body do not growth at the same rate. Scammon�s curve for growth shows 4 major tissue system of the body;
� Neural
� Lymphoid�
� General: Bone, viscera, muscle.
� Genital
The graph indicates the growth of the neural tissue is complete by 6-7 year of age. General body tissue show an �S� shaped curve with showing of rate during childhood and acceleration at puberty. Lymphoid tissues proliferate to its maximum in late childhood and undergo involution. At the same time growth of the genital tissue accelerate rapidly.�
�
Theories of Tooth Movement
-
Pressure-Tension Theory:
- Concept: This theory posits that tooth movement occurs in response to the application of forces that create areas of pressure and tension in the periodontal ligament (PDL).
- Mechanism: When a force is applied to a tooth, the side of the tooth experiencing pressure (compression) leads to bone resorption, while the opposite side experiences tension, promoting bone deposition. This differential response allows the tooth to move in the direction of the applied force.
- Clinical Relevance: This theory underlies the rationale for using light, continuous forces in orthodontic treatment to facilitate tooth movement without causing damage to the periodontal tissues.
-
Biological Response Theory:
- Concept: This theory emphasizes the biological response of the periodontal ligament and surrounding tissues to mechanical forces.
- Mechanism: The application of force leads to a cascade of biological events, including the release of signaling molecules that stimulate osteoclasts (bone resorption) and osteoblasts (bone formation). This process is influenced by the magnitude, duration, and direction of the applied forces.
- Clinical Relevance: Understanding the biological response helps orthodontists optimize force application to achieve desired tooth movement while minimizing adverse effects.
-
Cortical Bone Theory:
- Concept: This theory focuses on the role of cortical bone in tooth movement.
- Mechanism: It suggests that the movement of teeth is influenced by the remodeling of cortical bone, which is denser and less responsive than the trabecular bone. The movement of teeth through the cortical bone requires greater forces and longer durations of application.
- Clinical Relevance: This theory highlights the importance of considering the surrounding bone structure when planning orthodontic treatment, especially in cases requiring significant tooth movement.
Factors to Consider in Designing a Spring for Orthodontic Appliances
In orthodontics, the design of springs is critical for achieving effective tooth movement while ensuring patient comfort. Several factors must be considered when designing a spring to optimize its performance and functionality. Below, we will discuss these factors in detail.
1. Diameter of Wire
- Flexibility: The diameter of the wire used in the spring significantly influences its flexibility. A thinner wire will yield a more flexible spring, allowing for greater movement and adaptability.
- Force Delivery: The relationship between wire diameter and force delivery is crucial. A thicker wire will produce a stiffer spring, which may be necessary for certain applications but can limit flexibility.
2. Force Delivered by the Spring
-
Formula: The force (F) delivered by a spring can be expressed by the formula: [ $$F \propto \frac{d^4}{l^3} $$] Where:
- ( F ) = force applied by the spring
- ( d ) = diameter of the wire
- ( l ) = length of the wire
-
Implications: This formula indicates that the force exerted by the spring is directly proportional to the fourth power of the diameter of the wire and inversely proportional to the cube of the length of the wire. Therefore, small changes in wire diameter can lead to significant changes in force delivery.
3. Length of Wire
- Flexibility and Force: Increasing the length of the wire decreases the force exerted by the spring. Longer springs are generally more flexible and can remain active for extended periods.
- Force Reduction: By doubling the length of the wire, the force can be reduced by a factor of eight. This principle is essential when designing springs for specific tooth movements that require gentler forces.
4. Patient Comfort
- Design Considerations: The design, shape, size, and force generation of the spring must prioritize patient comfort. A well-designed spring should not cause discomfort or irritation to the oral tissues.
- Customization: Springs may need to be customized to fit the individual patient's anatomy and treatment needs, ensuring that they are comfortable during use.
5. Direction of Tooth Movement
- Point of Contact: The direction of tooth movement is determined by the point of contact between the spring and the tooth. Proper placement of the spring is essential for achieving the desired movement.
- Placement Considerations:
- Palatally Placed Springs: These are used for labial (toward the lips) and mesio-distal (toward the midline) tooth movements.
- Buccally Placed Springs: These are employed when the tooth needs to be moved palatally and in a mesio-distal direction.
Myofunctional Appliances
- Myofunctional appliances are removable or fixed devices that aim to correct dental and skeletal discrepancies by promoting proper oral and facial muscle function. They are based on the principles of myofunctional therapy, which focuses on the relationship between muscle function and dental alignment.
-
Mechanism of Action:
- These appliances work by encouraging the correct positioning of the tongue, lips, and cheeks, which can help guide the growth of the jaws and the alignment of the teeth. They can also help in retraining oral muscle habits that may contribute to malocclusion, such as thumb sucking or mouth breathing.
Types of Myofunctional Appliances
-
Functional Appliances:
- Bionator: A removable appliance that encourages forward positioning of the mandible and helps in correcting Class II malocclusions.
- Frankel Appliance: A removable appliance that modifies the position of the dental arches and improves facial aesthetics by influencing muscle function.
- Activator: A functional appliance that promotes mandibular growth and corrects dental relationships by positioning the mandible forward.
-
Tongue Retainers:
- Devices designed to maintain the tongue in a specific position, often used to correct tongue thrusting habits that can lead to malocclusion.
-
Mouthguards:
- While primarily used for protection during sports, certain types of mouthguards can also be designed to promote proper tongue posture and prevent harmful oral habits.
-
Myobrace:
- A specific type of myofunctional appliance that is used to correct dental alignment and improve oral function by encouraging proper tongue posture and lip closure.
Indications for Use
- Malocclusions: Myofunctional appliances are often indicated for treating Class II and Class III malocclusions, as well as other dental alignment issues.
- Oral Habits: They can help in correcting harmful oral habits such as thumb sucking, tongue thrusting, and mouth breathing.
- Facial Growth Modification: These appliances can be used to influence the growth of the jaws in growing children, promoting a more favorable dental and facial relationship.
- Improving Oral Function: They can enhance functions such as chewing, swallowing, and speech by promoting proper muscle coordination.
Advantages of Myofunctional Appliances
- Non-Invasive: Myofunctional appliances are generally non-invasive and can be a more comfortable option for patients compared to fixed appliances.
- Promotes Natural Growth: They can guide the natural growth of the jaws and teeth, making them particularly effective in growing children.
- Improves Oral Function: By retraining oral muscle function, these appliances can enhance overall oral health and function.
- Aesthetic Appeal: Many myofunctional appliances are less noticeable than traditional braces, which can be more appealing to patients.
Limitations of Myofunctional Appliances
- Compliance Dependent: The effectiveness of myofunctional appliances relies heavily on patient compliance. Patients must wear the appliance as prescribed for optimal results.
- Limited Scope: While effective for certain types of malocclusions, myofunctional appliances may not be suitable for all cases, particularly those requiring significant tooth movement or surgical intervention.
- Adjustment Period: Patients may experience discomfort or difficulty adjusting to the appliance initially, which can affect compliance.