NEET MDS Lessons
Orthodontics
Quad helix appliance is an orthodontic device used to expand the upper arch of teeth. It is typically cemented to the molars and features a U-shaped stainless steel wire with active helix springs, helping to correct issues like crossbites, narrow jaws, and crowded teeth. ### Components of the Quad Helix Appliance
-
Helix Springs:
- The appliance contains two or four active helix springs that exert gentle pressure to widen the dental arch.
-
Bands:
- It is attached to the molars using bands, which provide a stable anchor for the appliance.
-
Wire Framework:
- Made from 38 mil stainless steel wire, the framework allows for customization and adjustment by the orthodontist.
Functions of the Quad Helix Appliance
-
Arch Expansion:
- The primary function is to gradually widen the upper arch, creating more space for crowded teeth.
-
Correction of Crossbites:
- It helps in correcting posterior crossbites, where the lower teeth are positioned outside the upper teeth.
-
Molar Stabilization:
- The appliance stabilizes the molars in their correct position during treatment.
Indications for Use
-
Narrow Upper Jaw:
- Ideal for patients with a constricted upper arch.
-
Crowded Teeth:
- Used when there is insufficient space for teeth to align properly.
-
Class II and Class III Cases:
- Effective in treating specific malocclusions that require arch expansion.
Advantages of the Quad Helix Appliance
-
Non-Invasive:
- It is a non-surgical option for expanding the dental arch.
-
Fixed Design:
- As a fixed appliance, it does not rely on patient compliance for activation.
-
Customizable:
- The design allows for adjustments to meet individual patient needs.
Limitations of the Quad Helix Appliance
-
Initial Discomfort:
- Patients may experience mild discomfort or pressure during the first few weeks of use.
-
Oral Hygiene Challenges:
- Maintaining oral hygiene can be more difficult, requiring diligent cleaning around the appliance.
-
Adjustment Period:
- It may take time for patients to adapt to speaking and swallowing with the appliance in place.
Thumb Sucking
According to Gellin, thumb sucking is defined as �the placement of the thumb or one or more fingers in varying depth into the mouth.� This behavior is common in infants and young children, serving as a self-soothing mechanism. However, prolonged thumb sucking can lead to various dental and orthodontic issues.
Diagnosis of Thumb Sucking
1. History
- Psychological Component: Assess any underlying psychological factors that may contribute to the habit, such as anxiety or stress.
- Frequency, Intensity, and Duration: Gather information on how often the child engages in thumb sucking, how intense the habit is, and how long it has been occurring.
- Feeding Patterns: Inquire about the child�s feeding habits, including breastfeeding or bottle-feeding, as these can influence thumb sucking behavior.
- Parental Care: Evaluate the parenting style and care provided to the child, as this can impact the development of habits.
- Other Habits: Assess for the presence of other oral habits, such as pacifier use or nail-biting, which may coexist with thumb sucking.
2. Extraoral Examination
- Digits:
- Appearance: The fingers may appear reddened, exceptionally clean, chapped, or exhibit short fingernails (often referred to as "dishpan thumb").
- Calluses: Fibrous, roughened calluses may be present on the superior aspect of the finger.
- Lips:
- Upper Lip: May appear short and hypotonic (reduced muscle tone).
- Lower Lip: Often hyperactive, showing increased movement or tension.
- Facial Form Analysis:
- Mandibular Retrusion: Check for any signs of the lower jaw being positioned further back than normal.
- Maxillary Protrusion: Assess for any forward positioning of the upper jaw.
- High Mandibular Plane Angle: Evaluate the angle of the mandible, which may be increased due to the habit.
3. Intraoral Examination
-
Clinical Features:
- Intraoral:
- Labial Flaring: Maxillary anterior teeth may show labial flaring due to the pressure from thumb sucking.
- Lingual Collapse: Mandibular anterior teeth may exhibit lingual collapse.
- Increased Overjet: The distance between the upper and lower incisors may be increased.
- Hypotonic Upper Lip: The upper lip may show reduced muscle tone.
- Hyperactive Lower Lip: The lower lip may be more active, compensating for the upper lip.
- Tongue Position: The tongue may be placed inferiorly, leading to a posterior crossbite due to maxillary arch contraction.
- High Palatal Vault: The shape of the palate may be altered, resulting in a high palatal vault.
- Intraoral:
-
Extraoral:
- Fungal Infection: There may be signs of fungal infection on the thumb due to prolonged moisture exposure.
- Thumb Nail Appearance: The thumb nail may exhibit a dishpan appearance, indicating frequent moisture exposure and potential damage.
Management of Thumb Sucking
1. Reminder Therapy
- Description: This involves using reminders to help the child become aware of their thumb sucking habit. Parents and caregivers can gently remind the child to stop when they notice them sucking their thumb. Positive reinforcement for not engaging in the habit can also be effective.
2. Mechanotherapy
- Description: This approach involves using mechanical
devices or appliances to discourage thumb sucking. Some options include:
- Thumb Guards: These are devices that fit over the thumb to prevent sucking.
- Palatal Crib: A fixed appliance that can be placed in the mouth to make thumb sucking uncomfortable or difficult.
- Behavioral Appliances: Appliances that create discomfort when the child attempts to suck their thumb, thereby discouraging the habit.
Tweed's Analysis
Tweed's analysis is a comprehensive cephalometric method developed by Dr. Charles Tweed in the mid-20th century. It is primarily used in orthodontics to evaluate the relationships between the skeletal and dental structures of the face, particularly focusing on the position of the teeth and the skeletal bases. Tweed's analysis is instrumental in diagnosing malocclusions and planning orthodontic treatment.
Key Features of Tweed's Analysis
-
Reference Planes and Points:
- Sella (S): The midpoint of the sella turcica, a bony structure in the skull.
- Nasion (N): The junction of the frontal and nasal bones.
- A Point (A): The deepest point on the maxillary arch between the anterior nasal spine and the maxillary alveolar process.
- B Point (B): The deepest point on the mandibular arch between the anterior nasal spine and the mandibular alveolar process.
- Menton (Me): The lowest point on the symphysis of the mandible.
- Gnathion (Gn): The midpoint between Menton and Pogonion (the most anterior point on the chin).
- Pogonion (Pog): The most anterior point on the contour of the chin.
- Go (Gonion): The midpoint of the contour of the ramus and the body of the mandible.
-
Reference Lines:
- SN Plane: A line drawn from Sella to Nasion, representing the cranial base.
- Mandibular Plane (MP): A line connecting Gonion (Go) to Menton (Me), which represents the position of the mandible.
- Facial Plane (FP): A line drawn from Gonion (Go) to Menton (Me), used to assess the facial profile.
-
Key Measurements:
- ANB Angle: The angle formed between the lines
connecting A Point to Nasion and B Point to Nasion. It indicates the
relationship between the maxilla and mandible.
- Normal Range: Typically between 2� and 4�.
- SN-MP Angle: The angle between the SN plane and the
mandibular plane (MP), which helps assess the vertical position of the
mandible.
- Normal Range: Usually between 32� and 38�.
- Wits Appraisal: The distance between the perpendiculars dropped from points A and B to the occlusal plane. It provides insight into the anteroposterior relationship of the dental bases.
- Interincisal Angle: The angle formed between the long axes of the maxillary and mandibular incisors, which helps assess the inclination of the incisors.
- ANB Angle: The angle formed between the lines
connecting A Point to Nasion and B Point to Nasion. It indicates the
relationship between the maxilla and mandible.
-
Tweed's Philosophy:
- Tweed emphasized the importance of achieving a functional occlusion and a harmonious facial profile. He believed that orthodontic treatment should focus on the relationship between the dental and skeletal structures to achieve optimal results.
Clinical Relevance
- Diagnosis and Treatment Planning: Tweed's analysis helps orthodontists diagnose skeletal discrepancies and plan appropriate treatment strategies. It provides a clear understanding of the patient's craniofacial relationships, which is essential for effective orthodontic intervention.
- Monitoring Treatment Progress: By comparing pre-treatment and post-treatment cephalometric measurements, orthodontists can evaluate the effectiveness of the treatment and make necessary adjustments.
- Predicting Treatment Outcomes: The analysis aids in predicting the outcomes of orthodontic treatment by assessing the initial skeletal and dental relationships.
Mixed Dentition Analysis: Tanaka & Johnson Analysis
�This analysis is crucial for predicting the size of unerupted permanent teeth based on the measurements of erupted teeth, which is particularly useful in orthodontics.
Mixed Dentition Analysis
Mixed dentition refers to the period when both primary and permanent teeth are present in the mouth. Accurate predictions of the size of unerupted teeth during this phase are essential for effective orthodontic treatment planning.
Proportional Equation Prediction Method
When most canines and premolars have erupted, and one or two succedaneous teeth are still unerupted, the proportional equation prediction method can be employed. This method allows for estimating the mesiodistal width of unerupted permanent teeth.
Procedure for Proportional Equation Prediction Method
-
Measurement of Teeth:
- Measure the width of the unerupted tooth and an erupted tooth on the same periapical radiograph.
- Measure the width of the erupted tooth on a plaster cast.
-
Establishing Proportions:
- These three measurements form a proportion that can be solved to estimate the width of the unerupted tooth on the cast.
Formula Used
The following formula is utilized to calculate the width of the unerupted tooth:
[ Y_1 = \frac{X_1 \times Y_2}{X_2} ]
Where:
- Y1�= Width of the unerupted tooth whose measurement is to be determined.
- Y2�= Width of the unerupted tooth as seen on the radiograph.
- X1�= Width of the erupted tooth, measured on the plaster cast.
- X2�= Width of the erupted tooth, measured on the radiograph.
Application of the Analysis
This method is particularly useful in orthodontic assessments, allowing practitioners to predict the size of unerupted teeth accurately. By using the measurements of erupted teeth, orthodontists can make informed decisions regarding space management and treatment planning.
Growth is the increase in size It may also be defined as the normal� change in the amount of living substance. eg. Growth is the quantitative aspect and measures in units of increase per unit of time.
Development
It is the progress towards maturity (Todd). Development may be defined as natural sequential series of events between fertilization of ovum and adult stage.
Maturation
It is a period of stabilization brought by growth and development.
CEPHALOCAUDAL GRADIENT OF GROWTH
This simply means that there is an axis of increased growth extending from the head towards feet. At about 3rd month of intrauterine life the head takes up about 50% of total body length. At this stage cranium is larger relative to face. In contrast the limbs are underdeveloped.�
By the time of birth limbs and trunk have grown faster than head and the entire proportion of the body to the head has increased. These processes of growth continue till adult.��
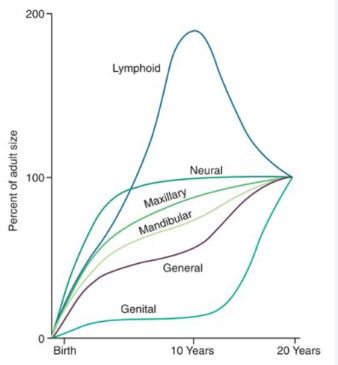
SCAMMON�S CURVE
In normal growth pattern all the tissue system of the body do not growth at the same rate. Scammon�s curve for growth shows 4 major tissue system of the body;
� Neural
� Lymphoid�
� General: Bone, viscera, muscle.
� Genital
The graph indicates the growth of the neural tissue is complete by 6-7 year of age. General body tissue show an �S� shaped curve with showing of rate during childhood and acceleration at puberty. Lymphoid tissues proliferate to its maximum in late childhood and undergo involution. At the same time growth of the genital tissue accelerate rapidly.�
�
Types of Springs
In orthodontics, various types of springs are utilized to achieve specific tooth movements. Each type of spring has unique characteristics and applications. Below are a few examples of commonly used springs in orthodontic appliances:
1. Finger Spring
- Construction: Made from 0.5 mm stainless steel wire.
- Components:
- Helix: 2 mm in diameter.
- Active Arm: The part that exerts force on the tooth.
- Retentive Arm: Helps retain the appliance in place.
- Placement: The helix is positioned opposite to the direction of the intended tooth movement and should be aligned along the long axis of the tooth, perpendicular to the direction of movement.
- Indication: Primarily used for mesio-distal movement of teeth, such as closing anterior diastemas.
- Activation: Achieved by opening the coil or moving the active arm towards the tooth to be moved by 2-3 mm.
2. Z-Spring (Double Cantilever)
- Construction: Comprises two helices of small diameter, suitable for one or more incisors.
- Positioning: The spring is positioned perpendicular to the palatal surface of the tooth, with a long retentive arm.
- Preparation: The Z-spring needs to be boxed in wax prior to acrylization.
- Indication: Used to move one or more teeth in the same direction, such as proclining two or more upper incisors to correct anterior tooth crossbites. It can also correct mild rotation if only one helix is activated.
- Activation: Achieved by opening both helices up to 2 mm at a time.
3. Cranked Single Cantilever Spring
- Construction: Made from 0.5 mm wire.
- Design: The spring consists of a coil located close to its emergence from the base plate. It is cranked to keep it clear of adjacent teeth.
- Indication: Primarily used to move teeth labially.
4. T Spring
- Construction: Made from 0.5 mm wire.
- Design: The spring consists of a T-shaped arm, with the arms embedded in acrylic.
- Indication: Used for buccal movement of premolars and some canines.
- Activation: Achieved by pulling the free end of the spring toward the intended direction of tooth movement.
5. Coffin Spring
- Construction: Made from 1.2 mm wire.
- Design: Consists of a U or omega-shaped wire placed in the midpalatal region, with a retentive arm incorporated into the base plates.
- Retention: Retained by Adams clasps on molars.
- Indication: Used for slow dentoalveolar arch expansion in patients with upper arch constriction or in cases of unilateral crossbite.
BONES OF THE SKULL
A) Bones of the cranial base:
A) Fontal (1)
B) Ethmoid (1)
C) Sphenoid (1)
D) Occipital (1)
B) Bones of the cranial vault:
1. Parietal (2)
2. Temporal (2)
C) Bones of the face:
Maxilla (2)
Mandible (1)
Nasal bone (2)
Lacrimal bone (2)
Zygomatic bone (2)
Palatine bone(2)
Infra nasal concha (2)
FUSION BETWEEN BONES
1. Syndesmosis: Membranous or ligamentus eg. Sutural point.
2. Synostosis: Bony union eg. symphysis menti.
3. Synchondrosis: Cartilaginous eg. sphenoccipital, spheno-ethmoidal.
GROWTH OF THE SKULL:
A) Cranium: 1. Base 2. Vault
B) Face: 1. Upper face 2.Lower face
CRANIAL BASE:
Cranial base grows at different cartilaginous suture. The cranial base may be divided into 3 areas.
1. The posterior part which extends from the occiput to the salatercica. The most important growth site spheno-occipital synchondrosis is situated here. It is active throughout the growing period and does not close until early adult life.
2. The middle portion extends from sella to foramen cecum and the sutural growth spheno-ethmoidal synchondrosis is situated here. The exact time of closing is not known but probably at the age of 7 years.
3. The anterior part is from foramen cecum and grows by surface deposition of bone in the frontal region and simultaneous development of frontal sinus.
CRANIAL VAULT:
The cranial vault grows as the brain grows. It is accelerated at infant. The growth is complete by 90% by the end of 5th year. At birth the sutures are wide sufficiently and become approximated during the 1st 2 years of life.
The development and extension of frontal sinus takes place particularly at the age of puberty and there is deposition of bone on the surfaces of cranial bone.